This blog is presented in fulfillment of the course requirements for SP208 Health Psychology (Sep - Oct 2015), Bachelor of Arts (Hons) Psychology, UCSI University, Malaysia.
Risk factors are not the immediate cause for a disease, it is a promoter, initiator, and the trigger for the occurrence of the disease (Bonomo & Araujo, 2012).
-Keep
and follow your medical appointments. Bring your medication along as it helps
ensure the doctor on what medication you are taking.
-Follow
the doctor’s instructions when consuming any medication. Be it,
over-the-counter medicine, cold or flu tablets, and nutritional supplements.
-Mention
all your side effects from any medication consumed. For example, the feeling of
depression and palpitations.
-If
you are having an arrhythmia symptoms, a new symptom or the symptom worsen, inform
the doctor.
-Take
care of yourself. Lie down if you are feeling light-headed.
-Consume
a healthy diet. Most arrhythmia cases are caused by underlying heart diseases.
Have a diet that consist plenty of fruits, vegetables, and whole grains. Commit
to physical activities regularly.
-Consume
healthy fats. As an example, olive oil, seeds and nuts. Omega-3s are found in
foods like tuna, sardine, salmon and flaxseeds.
Don’ts
-No
smoking.
-Caffeine,
alcohol and substances that can trigger arrhythmia. Caffeine is closely
associated with arrhythmia-particularly with fast heart beat
-Eat
food that are high in sodium. Salt increases blood pressure, which will then
increases the chances of having arrhythmia. Limit yourself to not consume more
than 1 5000 milligrams of sodium a day.
-Keep
away from animal fats.
-Foods
that are high in tyramine. Tyramine is a substance that are found in aged and
fermented foods. A few examples are aged cheeses (Cheddar), cured meats
(dry-type summer sausages), fermented cabbage (kimchee), certain sauces (soy
sauce) and yeast extract spreads (Marmite).
From the dos and don’ts patients can apply another
health behaviour theory can be applied to enhance adherence, for instance the transtheoretical model for stop
smoking orstop consuming excessive
amount of coffee or stop eating high-calorie foods. All of those are the
triggers of arrhythmia, thus it needs to control and stop.Let’s take coffee as an example; the patient
will start at the pre-contemplation stage, where he/she has no intention of
stopping his/her excessive intakes of coffee. Then he/she will start to feel
that there is fluttering action of his/her heart and realizing that the
excessive amount of coffee is the cause. This is the stage when he/she starts
to contemplate and wants to stop drinking too much coffee. The next stage is
preparation, he/she will prepare a coffee flavoured sweets, which contains only
a small amount of caffeine, or a chewing gum to replace coffee. Then the action
stage, he/she may decrease the number of cups that he/she takes every day for
example, only one cup per day and to be taken only during breakfast is to be
accomplished in a month time. Then improve on the progress made by drinking
only five cups a week, only on weekdays. Lastly, he/she should maintain with
drinking 5 cups of coffee during weekdays for every week, while trying to avoid
tempting situations.
Based on the statistics by the
American Heart Association, there are 4 300 000 Americans that are diagnosed
with Arrhythmia and 630 000 of them are admitted annually. The most common kind
of Arrhythmia is the Atrial Fibrillation, where 2.2 million Americans are
diagnosed with that disease. 70% of people having Atrial Fibrillation are
between the ages of 65 to 85. Per year, there are more than 250 000 deaths per
year caused by Ventricular Fibrillation.
Case
Study
This case study is about Roger, who
is 58 years old and he had Atrial Fibrillation. Atrial Fibrillation is a type
of fast heart beat arrhythmia (Tachycardia). It is the most common type of
arrhythmia and it is when your heart does not pump regularly or work as
properly as it should. This causes a “fluttering” heart beat, irregular pulse
and in Roger’s case, having severe chest pains. He felt a lot of nerve activity
in his chest area. At first, the pain was only temporarily but as time goes by,
the symptoms increased and lasted longer. After five months, he could not take
the pain and decided to see his general practioner. His GP’s first reaction was
he taught that Roger is having a problem. Roger was taken aback as his family
has no history of any heart problem or diseases related to the heart. His first
question was, “how could that even be?”. His GP then recommended him to make an
appointment with a heart specialist at a hospital.
Within the next eight weeks, he met
a heart specialist. Roger then proceeded by showing all his medical records and
check-ups with is GP. The heart
specialist first reaction is that his heart problem could be related to a heart
rhythm disturbance.
By the following month, he had two
Electrocardiograms (ECG), Echocardiogram, and a seven-day event recorder. After
the next meeting with the heat specialist, it is then confirmed that Roger is
having Arrhythmia and it is due to Paroxysmal Atrial Fibrillation. Paroxysmal
Atrial Fibrillation is when electrical signals in an individual’s heart causes
the heart to beat rapidly and it just stop on its own (Case-Lo, 2013). At
first, the heart specialist prescribed medication to lower his blood pressure
but it did have very little positive effects on him. He was then given
anti-arrhythmic medication and beta-blockers. He felt good for the first ten
days as he did not experience any symptoms. Sadly, these medication made Roger
feel very tired and was unable to perform his daily activities and his job.
Besides that, he kept a diary to jot down he felt every day since the change of
medication. It was also to track his Atrial Fibrillation episodes over the
months and tried various medication of the different dosage. Although with all
the medication, he was still experiencing the symptoms even after meeting the
heart specialist eight months later. So he got another medication and this
time, he felt a lot of positive effect on him. It made a big and fast
improvement in Roger. Again, the medicine was also effective for a short period
of time and the symptoms kept coming back days after that. The heart specialist
then asked him to refer to a hospital that has an Electrophysiological
Cardiologist.
An Electrophysiological Cardiologist
are qualified to perform special tests on an individual’s heart electrical
system (Orenstein, 2011). For an example, electrophysiology study or an
ablation and these was what the Electrophysiological Cardiologist suggested
Roger to go through. He explained that is has a 70% probability of being a
success. Roger agreed and was ask to be on the waiting list for the procedure.
His medication was changed to the previous anti arrhythmic medication hoping
that the effects would last longer but he was still having symptoms and every
day became a struggle for him.
Roger received a letter from the
hospital with the date arranged for him to undergo the procedure. A week before
the date of the procedure, he was asked to be at the hospital for a
pre-admission check-up and give a 45 minute information session about the
procedure. A week later, he arrived to the hospital for a procedure called
Pulmonary Vein Isolation. He was given medication to relax him and the
procedure lasted for three hours.
After the procedure, he was sent to
a special care unit to recover for the first few hours after the procedure. His
recovery was good and uncomplicated and the doctors allowed him to go back the
next day. Roger had home rest for the first two weeks and still have to take
his medication for the next eight weeks.
Even years after the procedure, his symptoms
decreased and he is much better now. He still takes his medicationn to control
his high blood pressure but now he only goes to the hospital annually for a
review after the procedure. His symptoms then completely subsided.
For
bradycardia patients, doctors usually hold off any medications that slows their
heartbeat, and treat the conditions by implanting a permanent or temporary
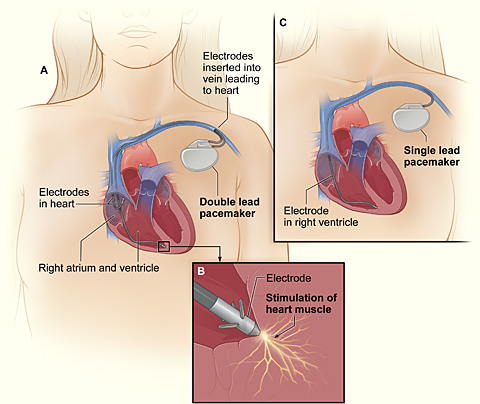
pacemaker(Arrhythmia Alliance, 2012). An artificial
pacemaker is a small battery operated device, that is approximately the size of
a fifty pence piece, used to detect and fires a small electrical impulse to
stimulate the heart wall to make it contract and to make the heart beats. It is
planted just under the skin of your chest (below your collar bone) and
insulated lead wires that connects to the pacemaker are attached to the heart
to help your heart muscle pump blood regularly (National
Heart Foundation Australia, 2015;Adelaide-Meath National Children's Hospital,
2015) . The lead also provides the information on the heartbeat’s
natural activity. The body will not reject artificial pacemaker.
Tachycardia: Vagal Maneuvers,
Cardioversion, Catheter Ablation and Pharmacological Medications
Vagal maneuver is a set of physical activities that stimulate the Vagus
nerve, the nerve serving
the structures of the chest, abdomen, head and neck, which supplies
parasympathetic impulses to the myocardium (heart muscle) and trigger the release of acetylcholine to put halt on the conduction of electrical impulses and decrease
the rapidity of the heart (Healthwise
Staff, 2012;Wang & Estes, 2014). The
maneuvers are gagging, holding your breath and bearing down (Valsalva
maneuver), immersing your face in ice-cold water (diving reflex), coughing and
Carotid massage (neck massage).
figure 2. Cardioversion
Cardioversion uses electrode patches to deliver a split-second energetic
shock to the heart muscles while the patient is sleeping, the shock applied
will interrupt the abnormal heart rhythm and return a normal heartbeat (Intermountain Healthcare, 2011;Texas Cardiac
Arrhythmia Institute, 2015;Tandri, 2015). This quick procedure may need
to be repeated to effectively restore a normal heart rhythm under the direction
of a team of highly trained doctors, nurses and technologists in the
electrophysiology lab(Intermountain Healthcare, 2011).
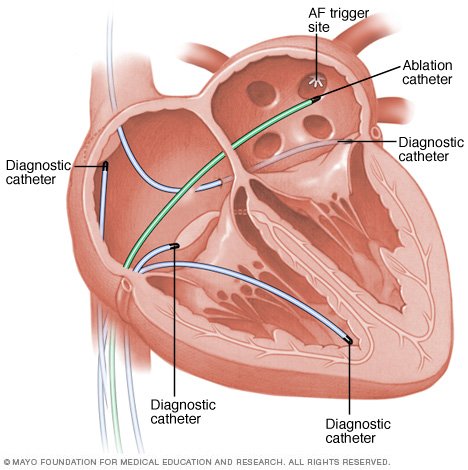
figure 3. Catheter Ablation
Catheter ablation uses radiofrequency energy to destroy (ablate) a small area of
the tissue of the heart which is causing arrhythmia. Guided with x-rays, the
doctor will insert several small catheters (thin, flexible tubes) through the
veins in the groin or neck and direct them to the tissues that interrupt the
heart’s electrical activity then thermal energy (extreme heat) or cryoenergy
(extreme cold) energy will be emitted to the problematic tissues through one of
the catheters (National Institute of Health,
2012;American Heart Association, 2014;Cleveland Clinic, 2015;Ashikaga, 2015).
This energy also disconnects the electrical pathway of the abnormal rhythm.
There are three main pharmacological drugs being prescribed
to an arrhythmic patient, they are the anti-arrhythmic drugs, the calcium
channel blockers and beta-blockers (American
Heart Association, 2014;Healthline Networks, 2015). Anti-arrhythmic drugs either cease the abnormal transmission of
electrical impulses send by the natural pacemaker tissue that is firing too
fast to the heart tissues(American Heart Association, 2014). The drugs are in a
form of pills or in a form of intravenous (IV) drip, they work to correct and
restore the normal rhythm of the heart. Next is the calcium channel blockers, which is also known as "calcium
antagonists." Calcium is an electrolyte that functions as the heart
regulator, imbalance of calcium will cause arrhythmia. Thus, calcium channel
blockers work by blocking the movement of the calcium electrolytes into the
heart and blood vessel tissue(Healthline Networks, 2015). It can be taken in
a form of pill or in a form of intravenous (IV) drip.Lastly,
beta-blockers, which is also known as ‘beta-adrenoceptor blocking’ that blocks adrenaline hormones from
stimulating rapid firing of electrical impulses to the heart tissues,
thus results in a decrease of heart beats, reduction of cardiac stress output
and lessening of the arterial blood pressure(Healthline Networks, 2015).
Bradycardia and
Tachycardia: Implantable Cardioverter Defibrillator (ICD) and Surgeries
figure 4. ICD
Implantable
Cardioverter Defibrillator (ICD) monitors the heartbeat constantly and automatically will detect
any irregular heart followed by a short electrical shock to the heart to
sustain a normal heart rate(Cheng, 2015). The shock is
generally expressed by patients as being “kicked in the chest,” as it gives a
momentary chest pain. The device must be check and/or replaced every four
months. It consists of a titanium-encased pulse generator (the size of a small
box of raisins) that contains a lithium battery and electrical circuitry and
capacitors attached to one, two or three leads (wires) that are inserted into
the heart and it is implanted under the skin beneath the collarbone(Cheng, 2015).
Two of the main surgeries for treating arrhythmia are the maze procedures and
coronary artery bypass grafting (CABG) surgery (University of California San
Francisco, 2015).
Maze surgery treats arrhythmia by making small cuts or burns in the heart tissues
that will prevent the transmission of abnormal electrical signals or by making
a "maze" of new electrical routes to let electrical impulses move
easily to the heart tissues (Texas Heart
Institue, 2015;University of California San Francisco, 2015). CABG is
when a healthy artery or vein is extracted from other parts of the body grafted
in between the blocked coronary artery, thus creating a new route for blood to
move to the heart tissues(National Institute of Health,
2012).
Adherence to Medical Advices and Preventive Measures
The most important
part that an arrhythmic patient needs to adhere is to follow the timeliness of
the medicated drug prescribed and to check the functionality of the planted
devices if they previously underwent those procedures. This is to prevent
arrhythmia to advance into a heart attack or a stroke.
As for the medication,
the patient can monitor their consumption by relying to the device called Medication Event Monitoring System (MEMS).
MEMS is a tracking medication usage device without any active patient input. It
consists of an electronic memory integrated into a cap designed to fit a normal
medicine bottle, it records the number of act on when the cap is opened to
remove a pill(Brannon & Feist, 2014).
The health belief model can also be applied,
from the previous consultations with the doctors; patients should already know
the fact that they are susceptible
in getting a heart attack or stroke as they are already arrhythmic. With that
they will come to acknowledge the severity
of getting a heart attack or stroke. Following that, they would search and take
the initiative to know more on how to improve their conditions and to maintain
it that way, in which it is their way of perceiving the benefits of health-enhancing behavior. Lastly, knowing their limits
for the level of exercising or kinds of foods that they can eat without
reaching the excess point is their way of perceiving barriers towards the health-enhancing behaviors(Brannon &
Feist, 2014).
For example, exercising too much may cause their heart to beat faster than
usual or eating too much omega-3 rich foods may cause electrolyte imbalance.
Arrhythmia divided into
two categories which is the ventricular arrhythmia and supraventricular
arrhythmia, (Texas Heart Institute,2015). The ventricular arrhythmia take place
in the lower chambers of heart termed the ventricles. Meanwhile,
supraventricular arrhythmia take place in the area above the ventricles termed
the atria. The Bradycardia means that the heart beats is too slow and the
Tachycardia means that the heart beats too fast.
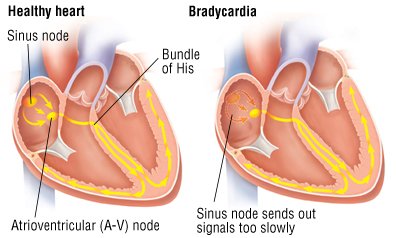
Bradycardia
figure 1. Bradycardia
Bradycardia is a slow
heart beat which is less than sixty beats per minute. This condition occurs
when the electrical impulse that signals the heart to contract is not formed in
the heart’s natural pacemaker which is the sinoatrial node, or it is not sent
to the ventricles, (University Hospital Southampton,2015). This type of
arrhythmia usually affects elderly people, but there are chances to affect
young generations as well. This condition is caused by any one of two factors
which is the central nervous system does not signal that the heart requires to
pump more or it could be due to the damage of sinoatrial node. The damage of
sinoatrial damage could be associated to aging, congenital defects, heart
diseases or medicines that is taken to control high blood pressure and
arrhythmia.
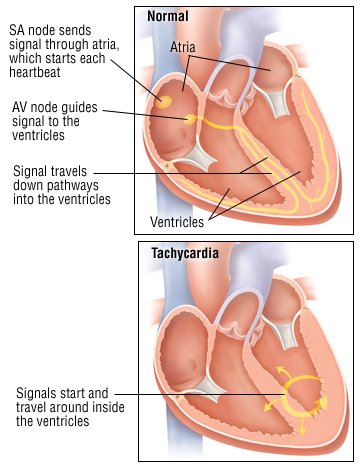
Tachycardia
figure 2. Tachycardia
Tachycardia is a fast
heart beat which is more than 100 beats per minute. There are few types of
tachycardia which depends on where the fast heart beat originates, (Mayo
Clinic, 2015). If the fast heart beat originates in the ventricles, it is
called the ventricular tachycardia. Meanwhile, if the fast heart beat
originates above the ventricles, it is called the supraventricular tachycardia.
Ventricular Arrhythmias
In ventricular
arrhythmias it consists of Ventricular Tachycardia, Ventricular Fibrillation,
and Premature Ventricular Contractions, (Texas Heart Institution, 2015). . The
ventricular tachycardia is a state in which the sinoatrial node no longer
controls the pounding of the ventricles and the pacemaker’s role is being taken
by the other parts alongside the lower electrical pathway. Since the signal
does not move through your heart muscle along the usual route and this
condition causes the heart muscle does not beat normally. Thus, this condition
would make a person feel as if their heart skip beats and this rhythm cause
severe shortness of breath, syncope or fainting.
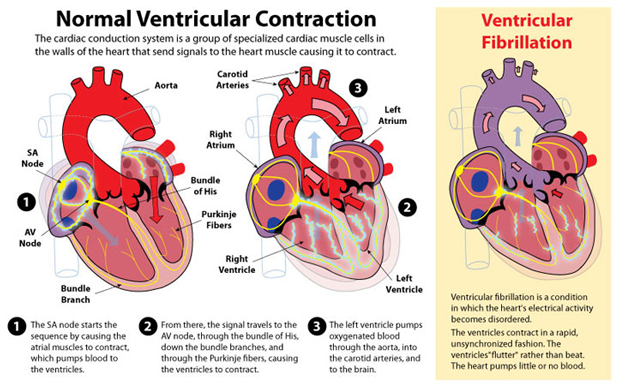
Ventricular Fibrillation
figure 3. Ventricular Fibrillation
The most serious type of
arrhythmia which results from an uncontrolled and irregular beat. A person who
suffers from ventricular fibrillation would have numerous impulses that arise
at the same time from various locations, (American Heart Association,n.d.). The
heartbeat sometimes could reach about 300 beats per minute and may face chaotic
heartbeat which means a very little amount of blood is being pumped from the
heart to the brain and body and might result in collapsing. Apart from that,
individuals who have history of heart attack or heart disease have a high risk
of getting ventricular fibrillation.
Premature Ventricular
Contractions
Premature Ventricular
Contractions also known as Premature Ventricular Beat is a less serious sort of
ventricular arrhythmia. According to Kulick and at el. (2015), this condition
occurs when ventricles contract rapidly out of order with the regular
heartbeat. Normally there is no treatment is needed for this condition but if
the individual have a history ventricular tachycardia or heart disease, it might cause
a serious type of arrhythmia. This condition could be caused by caffeine and
over-the-counter cold and cough medicine.
Supraventricular
Arrhythmias
In supraventricular
arrhythmias it consists of Supraventricular Tachycardia also known as
Paroxysmal Supraventricular Tachycardia, Atrial Fibrillation,
Wolff-Parkinson-White Syndrome, and Postural Orthostatic Tachycardia Syndrome,
(Texas Heart Institution, 2015). The supraventricular arrhythmia is a state
where it originates in the locations above the heart’s lower chambers which is
the atria or the atrial condition pathways. This condition, may or may not need
treatments and it might be caused by caffeine, alcohol, tobacco or cold and
cough medicines. Moreover, this condition would symptoms such as heart
palpitations, shortness of breath, chest tightness and a very fast pulse rate.
Supraventricular
Tachycardia or Paroxysmal Supraventricular Tachycardia
figure 4. Supraventricular Tachycardia
The supraventricular
tachycardia is a condition where regular and rapid heart rate from 150 to 250
beats per minute which beats in the atria. Meanwhile, in the paroxysmal
supraventricular tachycardia the word paroxysmal means irregularly or from time
to time. This condition occurs when the electrical signals in the heart’s upper
chambers fire peculiarly, which interferes with the electrical signals that
comes from the sinoatrial node and the beats in the atria eventually speeds up
the heart rate, (John Hopkins Medicine, n.d.). This condition normally common
among infants, young people and most likely to happen in anxious youngsters,
women and individuals who are very worn-out. Other than that, chain smokers,
alcoholic and individuals who takes coffee regularly have a higher risk.
Atrial Fibrillation
figure 5. Atrial Fibrillation
The atrial fibrillation
is a fast and irregular rhythm in which single muscle fibers in heart contract
or twitch, (National Health Service, 2015). This condition might cause the
blood to pool in the heart’s upper chambers and the pooled blood could lead to
blood clot. Once the blood clot travels from the heart and blocks the smaller
artery in the brain, stroke might take place. Thus, when an individual with
atrial fibrillation suffers from stroke, they may need antiplatelet therapy
which could prevent the formation of blood clot and causes stroke.
Wolff-Parkinson-White-Syndrome
figure 6. Woff-Parkinson-White-Syndrome pathway
The
Wolff-Parkinson-White (WPW) syndrome is a cluster of abnormalities caused by
additional muscle pathways amid the ventricles and the atria, (John Hopkins
Medicine,n.d.). This pathways cause the electrical signals to reach at the
ventricles too quickly, and the signals are sent back to the atria. Thus, it
resulted a very fast heart rate. Individuals with this syndrome might have
symptoms such as dizziness, episodes of fainting, chest palpitations and they
are most likely to have episodes of paroxysmal supraventricular tachycardia.
Postural orthostatic
tachycardia syndrome
figure 7. Effect of POTS to the body
Generally, when an
individual stands up, the body makes any desirable changes to compensate for
the gravitational stress of adjustment in body posture, (Dysautonomia
International, 2012). In order to keep the oxygen-rich blood flow to the brain
and the upper body, the heart rate increases and the blood vessels in the lower
part of body tighten. For some individuals, this does not occur and affect
their capability to stand or continue standing. This is called the orthostatic
intolerance. The postural orthostatic tachycardia syndrome is a type of
orthostatic intolerance. The patients with this condition, the blood vessels in
the lower body do not tighten when they are standing because
of the gravity causes
more blood to flow than normal moves to the lower body. Individuals with this
condition may have symptoms such as blurry vision, fatigue, headaches,
lightheadedness and fainting.
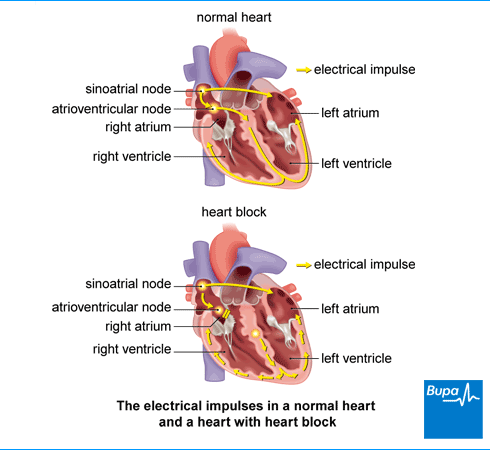
Heart Block
figure 8. Heart Block
The Heart block occurs
when the sinoatrial node sends its electrical signal appropriately, but the
signal is not sent via the atrioventricular, (Texas Heart Institute,2015). The
condition is most likely caused by aging or by the scarring or swelling of the
heart which at times results from the coronary artery disease. Moreover, it
could be caused by the cardiac amyloidosis, that is a condition where the
amyloid deposits take of the regular heart muscle.
According to National Health
Service (2014), there are few types of heart block, and named according to the
degree of severity.
First-Degree Heart
Block.
figure 9. First-Degree Heart Block
The first-degree heart
block means that the impulses are travelling via the atrioventricular node too
slowly.
Second-Degree Heart
Block
The second-degree heart
block means that the impulses are moving via the heart's atria but are deferred
in the atrioventricular node. Due to this delay the ventricles do not beat at
the right time.
Third-Degree Heart Block
The third-degree heart
block means that no impulses are reaching to the ventricles. In order to
make-up for this, the ventricles use its own backup pacemaker by way of its
slower rate. As a gap
in time is probable to
happen among the impulse from the atria and the impulse from the backup
pacemaker in the ventricles, an individual might faint. This situation is known
as a Stokes-Adams attack. The third-degree heart block is very severe and could
lead to heart failure or death.
Once the patient reported
that they have all the symptoms, they then will be referred to a Cardiologist
for further checkup and diagnosis to determine that if they suffer from
arrhythmia. The patient will undergo series of diagnosing process such as:
Blood Test
figure 1. Blood is drawn from a patient
Blood will be drawn from
their vein and sent to lab to check the level of substances in the blood such
as potassium. Potassium is an electrolyte that sends electrical impulses in the
heart for them to beat and pump the blood throughout the body (University of
Maryland Medical Center, 2015). High level of potassium increases the chances
of getting an arrhythmia because it sends excessive electrical impulses
(Nhs.uk, 2015).
Electrocardiogram (ECG)
figure 2. Patient undergoing ECG
This is a standard
cardiology tool for recording heartbeats and its rhythm. It uses electrodes
that act as a sensor to detect the electrical activity of the heart. These
electrodes are attached to certain parts of the chest. Patterns seen on the ECG
could tell if there is a presence of arrhythmia through the irregular waves
that the heart created (Heartrhythmcharity.org.uk, 2015).
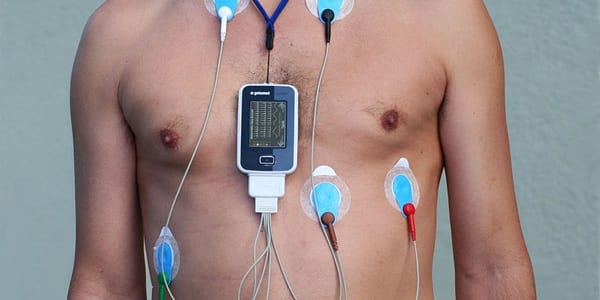
Holter Monitor
figure 3. Holter Monitor with ECG reading
This is a portable ECG
device that the patient attaches to their chest and it records the patient’s
heart rhythm as they go through their daily routine. They are asked to wear
this device for a day or more to see if they need to undergo more tests before
the cardiologist finally could determine what kind of treatment or medication
that they need (Heart.org, 2015).
Event Monitor
figure 4. An event monitor placed on patient
figure 5. Example of Event monitor
This portable device has
a similar function like a Holter Monitor, but the only difference is that the
patient will be asked to press a button on this device if they experience
arrhythmic symptoms so the cardiologist could check the heart rhythm at the
time of the symptom occurred (Bcpa.co.uk, 2015).
Echocardiogram
figure 6. Patient being diagnosed
This is another type of
cardiology tool. It is a noninvasive test that uses sound waves to produce
images of the patient’s heart’s size, structure and motion by placing a
transducer, a hand-held device on the chest (Mayoclinic.org,
2015).
Ambulatory
Electrocardiogram
This device has a
similar function as the Holter Monitor, where it tracks the heartbeat of the
patient but it is used only for 24 hours (WebMD.com, 2015)
If the arrhythmia did
not show up during those tests, the cardiologist will try to trigger the
arrhythmia using as follows:
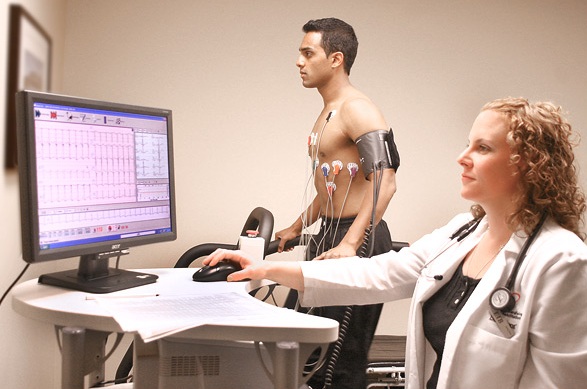
Stress Test
figure 7. Patient being assessed
During a stress test,
the patient will be asked to run on a treadmill or ride a stationary bicycle as
their heart activity is being monitored. The cardiologist may use a drug
instead to stimulate the heart in a way that is similar to exercise if the
cardiologist found out that the patient’s coronary artery disease caused the
arrhythmia, and they appeared to have a difficulty in exercising, (Nhs.uk,
2015).
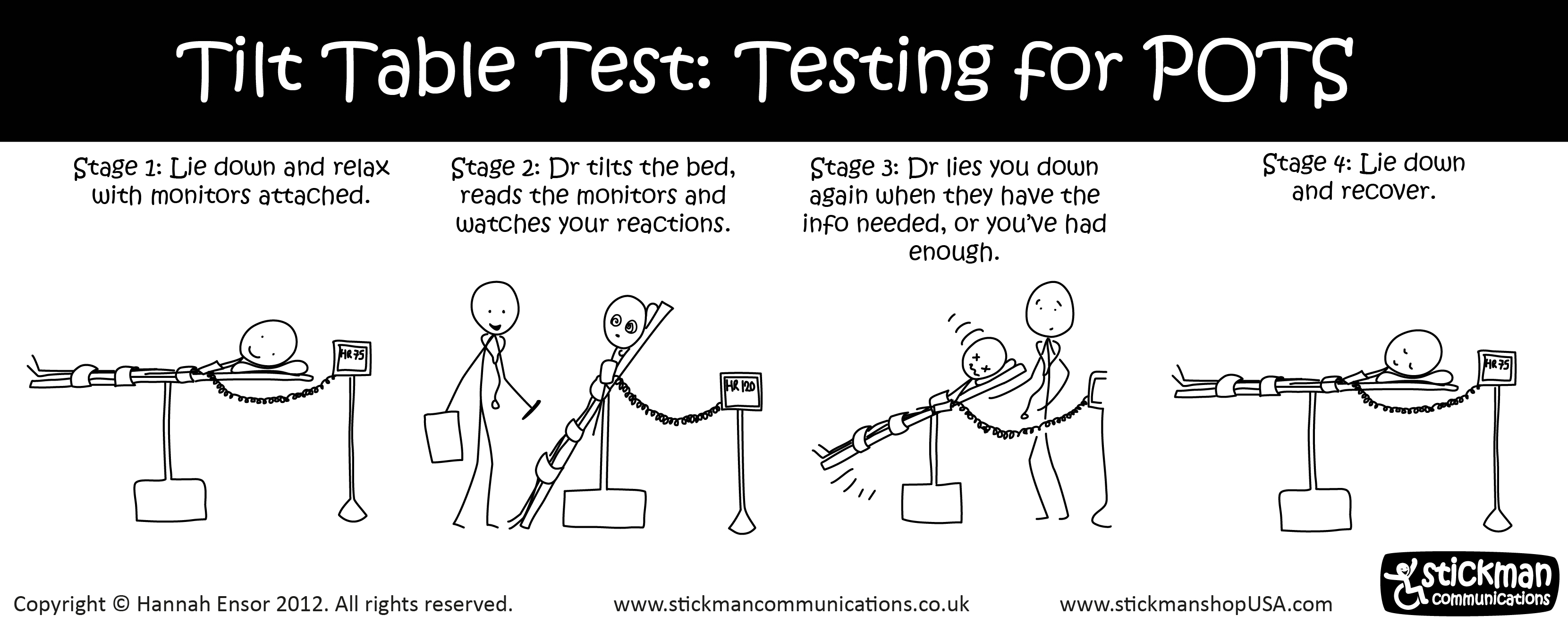
Tilt Table Test
figure 8. Process of Tilt Table Test
This type of test is
only used if the patient had a near fainting spell. The patient will be laid
flat on a table as their heart rate and blood pressure are being monitored.
Along the way, the table will be tilted to a standing position. The cardiologist
will observe how their heart and nervous system respond to the change in angle
(Nhs.uk, 2015).
Electrophysiological
Testing And Mapping.
figure 9. Placement of Catheter in the heart
figure 10. Electrophysiological test and Mapping in process
In this test, the
cardiologist will insert a thin thread, flexible tubes called catheter that are
tipped with electrodes through the patient’s blood vessels that are connected
to variety spots in their heart. The electrodes are used to map the spread of
electrical impulses throughout the patient’s heart. The cardiologist may also
use the electrodes to stimulate the patient’s heart to beat at rates that may trigger or halt
an arrhythmia. This enables the cardiologist to see the location of the
arrhythmia and determine what may be causing it (Nhs.uk, 2015).
Arrhythmias can produce
a broad range of symptoms, from barely perceptible to cardiovascular collapse
and death. When the arrhythmia occurs for longer time that it affects the
normal functioning, a more serious symptoms other than the irregular heartbeat,
may develop such as: (1) fatigue where they may experience extreme tiredness
(Merriam-webster.com, 2015), (2) dizziness where they experience a whirling
sensation in the head that may cause them to lose balance (Nhs.uk, 2015), (3)
lightheadedness where they feel dizzy and feel that they are about to pass out,
fainting or near fainting spells where they experience temporary loss of
consciousness (Heart.org, 2015), (4) shortness of breath where there is the
presence of sensation that they need extra effort to breath (Schueler, 2015)
and (5) chest pain. In a worst-case scenario, they may collapse and have sudden
cardiac arrest. Cardiac arrest is when someone collapsed in a sudden, is not
breathing normally and irresponsive because their heart suddenly stops pumping
blood to the whole body (Heart.org, 2015).
Risk factors are not the
immediate cause for a disease, it is a promoter, initiator, and the trigger for
the occurrence of the disease (Bonomo & Araujo, 2012). As for arrhythmia,
there are a number of cause for it to happen for instance, having coronary
artery disease, electrolyte imbalance in the body (lack or an excess of sodium
and potassium), changes in heart muscle, injury from heart attack and healing
after heart surgery (WEbMD, 2015). The factors leading to these causes are the
risk factors for arrhythmia. The risk factors are the socioeconomic status,
social support, age, gender, Type A Behavior Pattern (TABP), stress, Tako-Tsubo
syndrome and depression (Rozanski, Blumenthal & Kaplan, 1999).
Socioeconomic Status
(SES)
Socioeconomic status
determined the education, behavior and the cleanliness of the daily life.
According to a research done by Rozanski in 1999, low socioeconomic status has
a correlation with unhealthy behaviors and this increases the risk of having
coronary artery disease, which is one of the cause of arrhythmia. In addition
to that, low income restrict the health services they can get, lack of
education resulted in difficulties to adhere medical prescription and lack of
the consumption of nutritious foods. All these increases the potential of
getting a coronary artery disease and also electrolyte imbalance in the body,
in which both are the causes of arrhythmia.
Social Support
A population survey done
in America found that a significant relationship between coronary artery
disease and social support (Frasure-Smith & Lasperance, 1998). Social support
is the support you receive from friends, family and special people that care
for you (Towey et al.,
2013) and inhibition
from social support may lead to the causing factors of arrhythmia. Another
research done by Berkman and Syme (1979) reported that the number of social
ties correlates with the mortality rate and the mortality caused by coronary
artery disease was significantly related to the lack of social support. Social
support prevent the engagement of risky behaviors and biologically, it can decrease
the arterial pressure and cardiac response during stress (Bonomo & Araujo,
2012).
Age
Age is the major risk
factor for arrhythmia. This is because there is a decline in cardiac
functionality throughout the physiological aging (Bonomo & Araujo, 2012).
It was reported that out of a sample between the ages of 60 to 85 years old,
80% of them had ventricular arrhythmia and 88% of them had supraventricular
arrhythmia (Bonomo & Araujo, 2012).
Gender
Both male and female
have equal risk for arrhythmia but male are more prominent in the analysis of
most researches (Eaker, 1998). This is due to the biological differences
between genders in terms of hormonal composition, genetic inheritance and the
cerebral structure and functions. As for females, the pre-menopausal effect of
estrogen protect them from the risk of having coronary diseases (Bonomo &
Araujo, 2012). Thus protecting them from arrhythmia too.
Type A Behavior Pattern
(TABP)
Type A behavior pattern
is a set of behaviors of a person when confronting a challenging event (Bonomo
& Araujo, 2012). The characteristics are hostility, competitiveness,
impatience, rapidity and lack of attention to fatigue and sickness (Rozanski,
Blumenthal & Kaplan, 1999). People with this behavior pattern experiences
stress and thus affecting their cardiac activity and increases the arterial
pressure. Their inattention towards fatigue may also cause a biological haywire
such as platelets aggregation and intense discharge of the hormone
catecholamine (Bonomo & Araujo, 2012). Platelets accumulation may cause the
formation of plague in the artery which leads to coronary artery disease
(Brannon, Feist & Updegraff, 2014) and the hormone catecholamine increases
the heart beat in which will cause arrhythmia.
Stress
Stress is another major
risk factor for arrhythmia. The frequency of stressful events determined the
risk of heart diseases (Frasure-Smith & Lasperance, 1998). For example, the
stress from work will activate the sympathetic nervous system and promote the
increment of cardiac rate and arterial pressure, and lower the ejection of
blood from the heart (Bonomo & Araujo, 2012). This will interrupts the
cardiac activity and functionality and eventually cause arrhythmia.
Tako-Tsubo Syndrome
(Broken Heart Syndrome)
Tako-Tsubo syndrome
which is caused by the pressure in the apex of the ventricle of the heart due
to two factors; hormonal imbalance and stressful events (Bonomo & Araujo,
2012). This causes a person to have a symptom of chest pain. This syndrome
generally affects women after menopause who undergo some stressful episodes.
Continual application of pressure on the ventricle causes irregular heart beat
which is arrhythmia (Bonomo & Araujo, 2012).
Depression
Depression is the
feeling of sadness, loneliness, hopelessness, guilt and shame (Kubzansky &
Kawachi, 2000). Depression causes hormonal imbalance and inhibition from social
support thus leading its way to coronary and cardiac problems. A study by Lane
(2005) reported that 16% of the
patients diagnosed with moderate and severe depression experienced cardiac
events and he found that depressed patients have two times higher risk of
getting







.jpg)